Overview
Plantar fasciitis is a common and often persistent kind of repetitive strain injury afflicting runners, walkers and hikers, and nearly anyone who stands for a living – cashiers, for instance. It causes mainly foot arch pain and/or heel pain. Morning foot pain is a signature symptom. Plantar fasciitis is not the same thing as heel spurs and flat feet, but they are related and often confused. Most people recover from plantar fasciitis with a little rest, arch support (regular shoe inserts or just comfy shoes), and stretching, but not everyone. Severe cases can stop you in your tracks, undermine your fitness and general health, and drag on for years. This tutorial is mostly for you: the patient with nasty chronic plantar fasciitis that just won’t go away.
Causes
Training on improper, hard and/or irregular surfaces as well as excessive track work in spiked shoes, or steep hill running, can stress the plantar fascia past its limits of elasticity, leading to injury. Finally, failure in the early season to warm up gradually gives the athlete insufficient time for the structures of the foot to re-acclimate and return to a proper fitness level for intensive exercise. Such unprepared and repeated trauma causes microscopic tearing, which may only be detected once full-blown plantar fasciitis and accompanying pain and debilitation have resulted. If the level of damage to the plantar fascia is significant, an inflammatory reaction of the heel bone can produce spike-like projections of new bone, known as heel spurs. Indeed, plantar fasciitis has occasionally been refereed to as heel spur syndrome, though such spurs are not the cause of the initial pain but are instead a further symptom of the problem. While such spurs are sometimes painless, in other cases they cause pain or disability in the athlete, and surgical intervention to remove them may be required. A dull, intermittent pain in the heel is typical, sometimes progressing to a sharp, sustained discomfort. Commonly, pain is worse in the morning or after sitting, later decreasing as the patient begins walking, though standing or walking for long periods usually brings renewal of the pain.
Symptoms
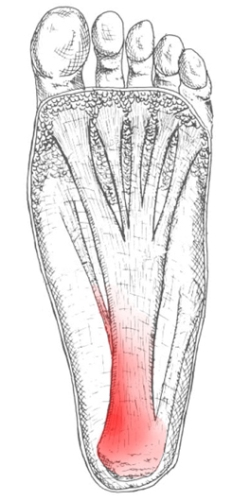
Plantar fascia usually causes pain and stiffness on the bottom of your heel although some people have heel spurs and suffer no symptoms at all. Occasionally, heel pain is also associated with other medical disorders such as arthritis (inflammation of the joint), bursitis (inflammation of the tissues around the joint). Those who have symptoms may experience ‘First step’ pain (stone bruise sensation) after getting out of bed or sitting for a period of time. Pain after driving. Pain on the bottom of your heel. Deep aching pain. Pain can be worse when barefoot.
Diagnosis
To arrive at a diagnosis, the foot and ankle surgeon will obtain your medical history and examine your foot. Throughout this process the surgeon rules out all the possible causes for your heel pain other than plantar fasciitis. In addition, diagnostic imaging studies such as x-rays or other imaging modalities may be used to distinguish the different types of heel pain. Sometimes heel spurs are found in patients with plantar fasciitis, but these are rarely a source of pain. When they are present, the condition may be diagnosed as plantar fasciitis/heel spur syndrome.
Non Surgical Treatment
Reducing inflammation in the plantar fascia ligament is an important part of treatment, though this does not address the underlying damage to the ligament. Initial home treatment includes staying off your feet and applying ice for 15 to 20 minutes three or four times a day to reduce swelling. You can also try reducing or changing your exercise activities. Using arch supports in your shoes and doing stretching exercises may also help to relieve pain. Nonsteroidal anti-inflammatory drugs (NSAIDS), such as ibuprofen (i.e. Motrin or Advil) and naproxen (i.e. Aleve), are often used to reduce inflammation in the ligament. If home treatments and over-the-counter anti-inflammatory drugs don’t ease the pain, an injection of a corticosteroid directly into the damaged section of the ligament can be given. Your doctor can do this in his or her office. Your doctor may use an ultrasound device to help determine the best place for the injection. Corticosteroids can also be administered on the skin of your heel or the arch of your foot, and then a painless electrical current is applied to let the steroid pass through your skin and into the muscle. Physical therapy is an important part of treatment for planter fasciitis. It can help stretch your plantar fascia and Achilles tendons. A physical therapist can also show you exercises to strengthen your lower leg muscles, helping to stabilize your walk and lessen the workload on your plantar fascia. If pain continues and other methods aren’t working, your doctor may recommend extracorporeal shock wave therapy. Sound waves are bombarded against your heel to stimulate healing within the ligament. This treatment can result in bruises, swelling, pain, and numbness, and has not been proven to be consistently effective in relieving symptoms.

Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
Prevention
Warm up properly. This means not only stretching prior to a given athletic event, but a gradual rather than sudden increase in volume and intensity over the course of the training season. A frequent cause of plantar fasciitis is a sudden increase of activity without suitable preparation. Avoid activities that cause pain. Running on steep terrain, excessively hard or soft ground, etc can cause unnatural biomechanical strain to the foot, resulting in pain. This is generally a sign of stress leading to injury and should be curtailed or discontinued. Shoes, arch support. Athletic demands placed on the feet, particularly during running events, are extreme. Injury results when supportive structures in the foot have been taxed beyond their recovery capacity. Full support of the feet in well-fitting footwear reduces the likelihood of injury. Rest and rehabilitation. Probably the most important curative therapy for cases of plantar fasciitis is thorough rest. The injured athlete must be prepared to wait out the necessary healing phase, avoiding temptation to return prematurely to athletic activity. Strengthening exercises. Below are two simple strength exercises to help condition the muscles, tendons and joints around the foot and ankle. Plantar Rolling, Place a small tin can or tennis ball under the arch of the affected foot. Slowly move the foot back and forth allowing the tin can or tennis ball to roll around under the arch. This activity will help to stretch, strengthen and massage the affected area. Toe Walking, Stand upright in bare feet and rise up onto the toes and front of the foot. Balance in this position and walk forward in slow, small steps. Maintain an upright, balanced posture, staying as high as possible with each step. Complete three sets of the exercise, with a short break in between sets, for a total of 20 meters.
 Overview
Overview Symptoms
Symptoms





 Your Achilles tendon is located at the back of your foot, just above your heel. It connects your heel to the two muscles of your calf and helps your foot push forward every time you take a step. If the tendon becomes swollen or irritated due to overuse, it can lead to the painful condition called Achilles tendonitis. If Achilles tendonitis goes untreated, it can become a chronic (ongoing) condition that makes just walking around almost impossible. Achilles tendonitis is a very common running injury. But it can also affect basketball players, dancers, or people who put a lot of repeated stress on their feet. It can be very painful.
Your Achilles tendon is located at the back of your foot, just above your heel. It connects your heel to the two muscles of your calf and helps your foot push forward every time you take a step. If the tendon becomes swollen or irritated due to overuse, it can lead to the painful condition called Achilles tendonitis. If Achilles tendonitis goes untreated, it can become a chronic (ongoing) condition that makes just walking around almost impossible. Achilles tendonitis is a very common running injury. But it can also affect basketball players, dancers, or people who put a lot of repeated stress on their feet. It can be very painful.







You must be logged in to post a comment.